You’ll need to suction your patient’s tracheostomy based on clinical indicators—not schedules—using appropriately sized catheters (12-16 Fr for adults) and regulated vacuum pressure (80-120 mmHg). Always perform hand hygiene, hyperoxygenate for 30-60 seconds, then insert the catheter without suction until you meet resistance. Withdraw 1-2 cm and apply intermittent suction while rotating during removal. Monitor continuously for complications including hypoxemia, bradycardia, and mucosal trauma. Understanding proper technique, equipment selection, and documentation standards guarantees you’ll minimize the 30% complication rate associated with improper procedures.
Key Takeaways
- Perform suctioning based on clinical indicators like visible secretions, coarse breath sounds, or decreased oxygen saturation, not on schedule.
- Use appropriately sized sterile catheters, not exceeding half the tracheostomy tube’s internal diameter, with suction pressure 80-120 mmHg for adults.
- Hyperoxygenate patient for 30-60 seconds before insertion, then insert catheter without suction until resistance, withdrawing 1-2 cm.
- Apply intermittent suction while rotating catheter during withdrawal, limiting each pass to prevent hypoxemia and mucosal trauma.
- Monitor oxygen saturation continuously, allow rest periods between attempts, and document pre-post assessments and secretion characteristics.
Indications and Assessment: When to Perform Tracheostomy Suctioning
Tracheostomy suctioning should be performed only when clinical indicators demonstrate secretion accumulation, not on a predetermined schedule.
You’ll need to assess specific indications criteria before intervening: visible secretions in the tube, coarse breath sounds during auscultation, increased peak airway pressures, decreased oxygen saturation, respiratory distress, or patient restlessness suggesting obstruction.
Your assessment tools include pulse oximetry monitoring, chest auscultation, and direct visualization of the tracheostomy site.
You must evaluate the patient’s work of breathing, noting accessory muscle use or paradoxical breathing patterns. Document baseline essential signs before suctioning.
Effective cough clearance may eliminate the need for intervention, so you’ll want to assess the patient’s ability to mobilize secretions independently.
This patient-centered approach prevents unnecessary trauma while ensuring adequate airway clearance when genuinely needed.
Essential Equipment and Supplies for Safe Suctioning
Before initiating tracheostomy suctioning, you’ll need to assemble sterile and non-sterile supplies that adhere to infection control standards. Your essential equipment includes sterile suction catheters sized appropriately for the tracheostomy tube (typically half the inner diameter), sterile gloves, and sterile normal saline for catheter irrigation.
Sterile technique is non-negotiable: properly sized catheters, sterile gloves, and saline irrigation form the foundation of safe tracheostomy suctioning.
You’ll require a regulated suction source with pressure settings between 80-120 mmHg for adults, ensuring equipment safety during the procedure.
Non-sterile supplies comprise clean gloves for your non-dominant hand, a face shield or goggles, and a disposable apron to maintain universal precautions. Keep supplemental oxygen readily available to prevent hypoxemia.
Proper suctioning techniques demand a sterile suction catheter for each pass, never reusing catheters between attempts. This systematic preparation protects your patient from infection while optimizing procedural effectiveness.
Selecting Appropriate Catheter Sizes and Vacuum Pressure Settings
While proper equipment preparation establishes the foundation for safe suctioning, selecting the correct catheter size and vacuum pressure directly impacts patient outcomes and airway integrity. Your catheter selection should never exceed half the tracheostomy tube’s internal diameter to prevent mucosal trauma and hypoxemia. Calculate this by multiplying the tube size by two, then selecting the next smallest catheter size.
| Patient Population | Recommended Catheter Size |
|---|---|
| Adult | 12-16 Fr |
| Pediatric | 8-10 Fr |
| Infant | 5-8 Fr |
| Neonatal | 5-6 Fr |
Vacuum settings require equal precision. You’ll maintain 80-120 mmHg for adults, 80-100 mmHg for children, and 60-80 mmHg for infants. These parameters minimize tissue damage while ensuring effective secretion removal through evidence-based practice protocols.
Step-by-Step Suctioning Procedure and Best Practices
Mastering the suctioning procedure demands systematic execution of twelve critical steps that safeguard patient airways while minimizing complications.
You’ll begin by performing hand hygiene and donning personal protective equipment. Hyperoxygenate your patient for 30-60 seconds before insertion.
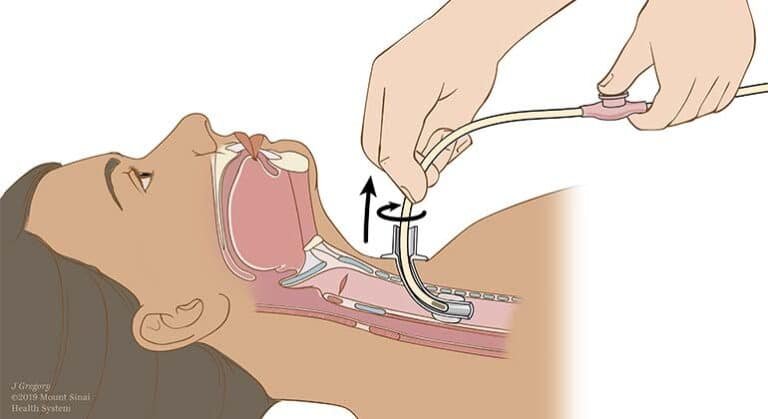
Using sterile suctioning techniques, insert the catheter without applying vacuum until resistance occurs, then withdraw 1-2 centimeters. Apply intermittent suction while rotating the catheter during withdrawal, limiting each pass to 10-15 seconds maximum.
Between attempts, allow adequate rest periods for reoxygenation. Monitor essential signs continuously, observing for bradycardia or desaturation.
Prioritize patient comfort through clear communication and gentle handling. Dispose of equipment properly, document secretion characteristics, and assess breath sounds post-procedure.
Your adherence to these evidence-based protocols directly impacts patient outcomes and recovery trajectories.
Pre-Oxygenation and Monitoring During the Procedure
Oxygen saturation maintenance represents the cornerstone of safe tracheostomy suctioning, requiring you to deliver supplemental oxygen at 100% FiO2 for 30-60 seconds prior to catheter insertion.
Pre oxygenation methods include ventilator adjustments, manual resuscitation bags, or oxygen flow increases through tracheostomy collars. You’ll prevent hypoxemia-related complications when implementing this protocol consistently.
Essential monitoring devices include pulse oximeters for continuous SpO2 tracking, cardiac monitors for heart rate assessment, and capnography when available.
You must observe your patient’s respiratory pattern, skin color, and level of consciousness throughout the procedure. Discontinue suctioning immediately if SpO2 drops below 90%, dysrhythmias develop, or severe distress occurs.
Resume pre-oxygenation between passes, allowing adequate recovery time before subsequent catheter insertions to protect your patient’s cardiopulmonary stability.
Complications, Warning Signs, and Risk Mitigation Strategies
Tracheostomy suctioning carries inherent risks that demand vigilant recognition and prompt intervention.
You’ll encounter potential complications including hypoxemia, bradycardia, bronchospasm, mucosal trauma, and infection. Your risk assessment must identify vulnerable patients—those with cardiac instability, hypoxemia, or bleeding disorders require heightened surveillance.
Monitor oxygen saturation continuously, maintaining levels above 90%. Implement strict aseptic technique to prevent healthcare-associated infections. Limit suctioning duration to 10-15 seconds, allowing recovery periods between passes.
You’ll mitigate trauma by avoiding excessive negative pressure and rigid catheter advancement against resistance.
Recognize warning signs immediately: persistent desaturation, arrhythmias, increased bleeding, or respiratory distress. Your complication management protocol should include emergency oxygen administration, procedure cessation, and physician notification.
Document all adverse events thoroughly, ensuring systematic quality improvement and enhanced patient safety through reflective practice modifications.
Documentation Requirements and Quality Improvement Considerations
Accurate documentation transforms tracheostomy suctioning from a routine procedure into legally defensible, quality-driven patient care.
You’ll need to record pre- and post-suctioning assessments, oxygen saturation levels, secretion characteristics, patient tolerance, and any adverse events. Documentation standards require time-stamping each intervention with specific details about catheter size, suction pressure settings, and number of passes performed.
You’re creating an evidence trail that supports clinical decision-making and protects both patient and provider.
Quality improvement initiatives depend on your meticulous record-keeping to identify trends, complications, and training needs.
Track infection rates, unplanned extubations, and patient outcomes systematically. Compare your unit’s metrics against established benchmarks, then implement targeted interventions.
You’ll contribute directly to advancing patient safety through data-driven practice modifications that elevate care standards.
Conclusion
You’ll maintain airway patency through systematic application of evidence-based suctioning protocols. Adhere strictly to sterile technique, appropriate catheter sizing, and safe vacuum pressure limits. You must monitor your patient’s oxygen saturation continuously and respond immediately to adverse signs. Document each procedure thoroughly, noting secretion characteristics and patient tolerance. Regular competency assessments and protocol reviews guarantee you’re delivering peak care while minimizing infection risk and tissue trauma. Your vigilance directly impacts patient outcomes.